Pharmacotherapeutic group: Analgesics; Other analgesics and antipyretics; Anilides.
ATC Code: N02BE01.
Pharmacology: Pharmacodynamics: Mechanism of action: The precise mechanism of the analgesic and antipyretic properties of paracetamol has still to be established; it may involve central and peripheral
actions.
Pharmacodynamic effects: Paracetamol provides onset of pain relief within 5 to 10 minutes after the start of administration. The peak analgesic effect is obtained in 1 hour and the duration of this effect is usually 4 to 6 hours.
Paracetamol reduces fever within 30 minutes after the start of administration with a duration of the antipyretic effect of at least 6 hours.
Pharmacokinetics: Adults: Absorption: Paracetamol pharmacokinetics is linear up to 2 g after single administration and after repeated administration during 24 hours.
The bioavailability of paracetamol following infusion of 500 mg and 1 g of Paracetamol is similar to that observed following infusion of 1 g and 2 g propacetamol (containing 500 mg and 1 g paracetamol respectively). The maximal plasma concentration (C
max) of paracetamol observed at the end of 15-minutes intravenous infusion of 500 mg and 1 g of Paracetamol is about 15 μg/ml and 30 μg/ml respectively.
Distribution: The volume of distribution of paracetamol is approximately 1 l/kg.
Paracetamol is not extensively bound to plasma proteins.
Following infusion of 1 g paracetamol, significant concentrations of paracetamol (about 1.5 μg/ml) were observed in the cerebrospinal fluid at and after the 20
th minute following infusion.
Biotransformation: Paracetamol is metabolised mainly in the liver following two major hepatic pathways: glucuronic acid conjugation and sulphuric acid conjugation. The latter route is rapidly saturable at doses that exceed the therapeutic doses. A small fraction (less than 4 %) is metabolised by cytochrome P450 to a reactive intermediate (N-acetyl benzoquinone imine) which, under normal conditions of use, is rapidly detoxified by reduced glutathione and eliminated in the urine after conjugation with cysteine and mercapturic acid. However, during massive overdosing, the quantity of this toxic metabolite is increased.
Elimination: The metabolites of paracetamol are mainly excreted in the urine. 90 % of the dose administered is excreted within 24 hours, mainly as glucuronide (60 - 80 %) and sulphate (20 - 30 %) conjugates. Less than 5 % is eliminated unchanged. Plasma half-life is 2.7 hours and total body clearance is 18 l/h.
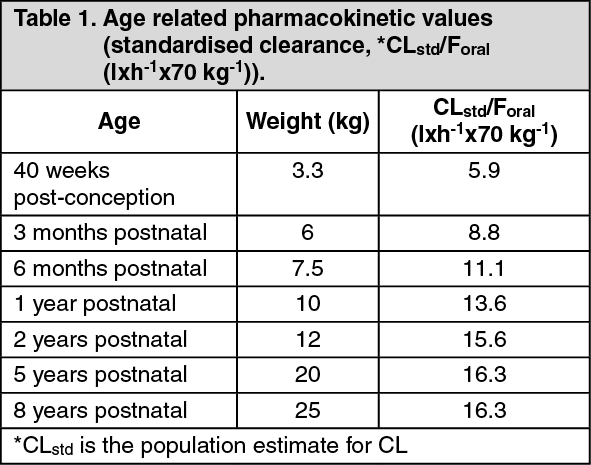
Newborn infants, infants and children: The pharmacokinetic parameters of paracetamol observed in infants and children are similar to those observed in adults, except for the plasma half-life that is slightly shorter (1.5 to 2 h) than in adults. In newborn infants, the plasma half-life is longer than in infants i.e. around 3.5 hours. Newborn infants, infants and children up to 10 years excrete significantly less glucuronide and more sulphate conjugates than adults. (See Table 1.)
 Click on icon to see table/diagram/image
Special populations:
Click on icon to see table/diagram/image
Special populations: Renal insufficiency: In cases of severe renal impairment (creatinine clearance 10 - 30 ml/min), the elimination of paracetamol is slightly delayed, the elimination half-life ranging from 2 to 5.3 hours. For the glucuronide and sulphate conjugates, the elimination rate is 3 times slower in subjects with severe renal impairment than in healthy subjects. Therefore when giving paracetamol to patients with severe renal impairment (creatinine clearance ≤ 30 ml/min), the minimum interval between each administration should be increased to 6 hours (see Dosage & Administration).
Elderly subjects: The pharmacokinetics and the metabolism of paracetamol are not modified in elderly subjects. No dose adjustment is required in this population.
Toxicology: Preclinical safety data: Non-clinical data reveal no special hazard for humans beyond the information included in other sections of the SmPC.
Studies on local tolerance of paracetamol in rats and rabbits showed good tolerability. Absence of delayed contact hypersensitivity has been tested in guinea pigs.
Conventional studies using the currently accepted standards for the evaluation of toxicity to reproduction and development are not available.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image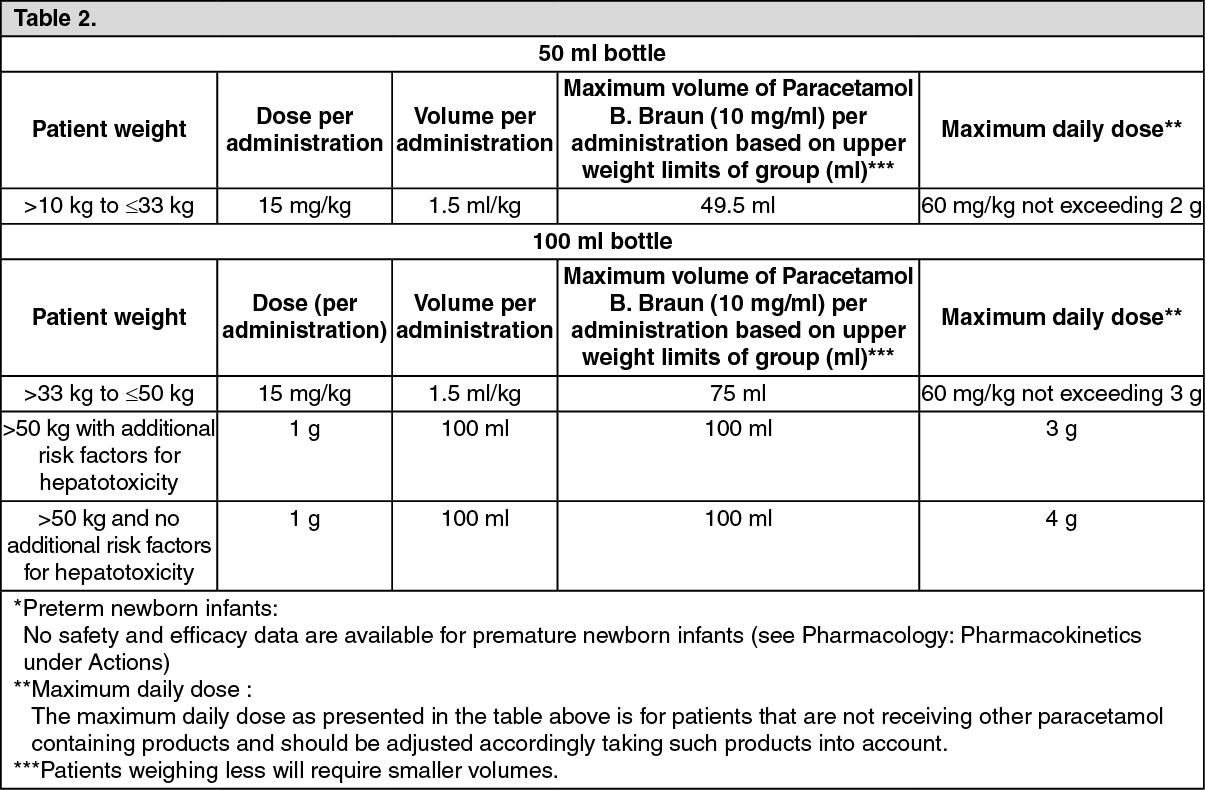 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out
